

. WPW isItself there is no abnormality of any human heart, but shows the specific ECG findings, that there is an interesting example of these ECG abnormalities are known to normalize from circa 1915 also suddenly, causing heart disease paroxysmal tachycardia often was (
Heart disease researcher in 1930, three named. White Wolff, Parkinson has collected 12 cases like this case, since the clinical findings reported in detail that, for example, electrocardiogram, the disease is an acronym for these three now referred to as taking the WPW syndrome. The photo below is a snapshot of 1955 is when Dr.White, visited the School of Medicine, Kyushu University for joint research international epidemiology of ischemic heart disease.
Features of the clinical picture of WPW syndrome are summarized in the following three points.
Indicate a specific type ECG WPW).
2) this WPW type ECG, suddenly to normal operation, or any kind of naturally.
Paroxysmal tachycardia heart 3), to merge a high rate of attacks, such as tachycardia) flutter (atrial fibrillation.
However, only shows the type ECG in WPW, There are also examples, such as normalization and does not attack case without tachycardia, but also by various operations. Type electrocardiogram shows only the
WPW, tachycardia cases without any attack is discovered incidentally in health screening and physical examination of the school.
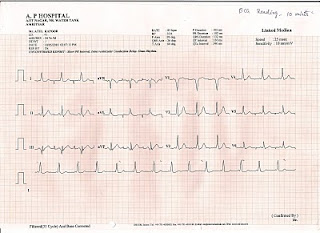
Two. ECG findings of WPW syndrome
And (electrocardiogram type WPW) is an electrocardiogram with the following features such as ECG findings characteristic of the syndrome WPW.
The emergence of wave 1) δ
Shorten the interval 2) PR
Interval prolongation 3) QRS
Often accompanied by changes in ST-T 4).
Three. Consists of normal electrocardiogram (link)
In order to understand the electrocardiogram of WPW syndrome, you need to understand the normal electrocardiogram. If you would like to know about your normal electrocardiogram Please see this link.
Four. Delta wave
. Sent out to ventricle the blood to contract atrium, found when send to systemic blood to contract ventricle, there was a difference some time between the contraction of the ventricle and atrial contraction, a lot of blood from the atrium to the ventricles and then is required for feeding can be, to maintain cardiac output more.
Five. Expansion of the QRS interval
If the second (0.05 to 0.10), and WPW syndrome is located on the ventricle of either pathway excitement through the conduction system stimulation of normal, so transmitted almost simultaneously in the ventricle left and right, QRS interval is only narrow, ventricle that is excited at an early stage. On the other hand, is so excited by the excitement the
rest of the ventricular portion of the ventricle was reached through the normal atrioventricular conduction system, the end of the ventricular activation time is the same as normal. As a result, ventricular activation time is longer, QRS interval is prolonged (seconds ≧ 0.12).
6. And migration (normal ECG) electrocardiogram ECG and normal atrioventricular conduction WPW type
Interval may be shortened PR, interval prolongation QRS, WPW type electrocardiogram showed a delta wave, a sudden change in the normal electrocardiogram. This is also available if you want to migrate naturally, in some cases caused by various drugs and operations. Time was not considered accessory c
onduction pathway is considered as the cause of WPW syndrome, this behavior is a curious phenomenon, and indeed, of interest to elucidate the pathophysiology of this syndrome has been aroused. However, can be explained very clearly considering this phenomenon is to be the genesis of this syndrome have accessory conduction pathway.
the bypass), the excitement is made to pass through only the atrioventricular conduction system successfully, the electrocardiogram is normal for some reason (such as changes in autonomic tone), and will not pass through the accessory pathway excitement. But there is a case of no action, or to normal ECG waveform, or even the type WPW, has been called an example of this is intermittent WPW syndrome (intermettent WPW syndrome)..
How to normalize the waveform WPW type has the following methods.
A frequent ECG recording
Holter ECG recording two
Exercise 3
His bundle pacing 5
6 Take a deep breath
Vagus nerve stimulation 7: carotid sinus massage, ocular pressure
Ranked # 8 orthostatic
Formation of a refractory period: electrical stimulation of the pathway near 9
The table below shows the test drug to convert (ECG normal) ECG normal ECG atrioventricular conduction type WPW.
How to use chemical name
Intravenous procainamide over 10mg/kg, 5 minutes
50 ~ 100mg intravenous lidocaine
Ajumarin 50mg, intravenous
Amyl nitrite inhalation
Using sublingual nitroglycerin
Disopyramide 50mg, intrav
enous slowly
1.2mg atropine sulfate, bolus
Tachycardia attack 7.
One of the clinical features of WPW syndrome tachycardia is to show the attack. Attack of tachycardia WPW syndrome is mostly supraventricular tachycardia paroxysmal, there is a (atrial flutter) to some paroxysmal atrial fibrillation. As the frequency of arrhythmia was WPW syndrome has been reported as shown below.
Few percent of cases the type of arrhythmia
Paroxysmal supraventricular tachycardia 22 52.4
14.3 6 paroxysmal atrial fibrillation
2 4.8 paroxysmal atrial flutter
4.8 2 frequent atria
l premature beat
A sub-ventricular rhythm 2.4
7 16.7 tachycardia of unknown
Paroxysmal supraventricular tachycardia in WPW syndrome, so that rotation can occur by a pathway that atrium → ventricle → → pathway → atrial atrioventricular node excitement, strictly speaking, should be called tachycardia atrioventricular reciprocating tachycardia is the pulse attack. In the accessory pathway is reported only in the direction atrium → ventricle the excitement, you may not tell the nature of the atrium → ventricle direction (unidirectional conduction). If you have the accessory conduction pathway like this, because the non-ictal ECG does not show the type WPW, it is only normal to record the electrocardiogram make the diagnosis of WPW sy
ndrome is extremely difficult. Said, "potential WPW syndrome (concealed WPW syndrome)" and a case like this, has become one of the important cause of supraventricular tachycardia. Shimomura, consider the mechanism of cardiac electrophysiological supraventricular tachycardia, shows the grades as shown in the table below.
/ WPW syndrome in the atrioventricular node
Reentry within the sinus node (in the atrium)
Increased automaticity re-entry
Potential overt
Number 37 46 32 4 4 例
% 30.1 37.4 26.0 3.3 3.3
Eight. The frequency and
pathophysiology of WPW syndrome
The frequency of WPW type ECG, so it is said that one in 800 people in the survey, such as population screening is not 600 it is not a disease so little. Since not have a diagnosis about the frequency of latent WPW syndrome, and electrophysiological testing is not carried out the heart, its exact frequency is unknown, also seems to be quite frequently-as shown in the table above.
In adults, the boundary between the atrium and ventricle is the part of the bundle except Hisu atrioventricular node, are blocked completely by connective tissue fibers that wheel, coupling between the two there is no muscle in general. However, in the prenatal development of annulus fibrosus is incomplete and this, coupled with lots of muscle remained. Syssarcosis state like this was also still remaining is the old pathway.
Below is a diagram showing the pathogenesis of syndrome model WPW.
C is a typical disease, atrial activation to form a delta wave causing the excitement of the early part of the ventricular muscle through the accessory pathway. On the other hand, the remaining myocardium was excited by stimulation through the normal atrioventricular conduction system. Therefore, the ventricle is excited by both normal atrioventricular conduction system and accessory
pathway, to form a ventricular fusion beat.
3 shows the type of ventricular preexcitation syndrome caused by it and the type of accessory conduction pathway in the figure below.
3 type of accessory pathway
AVN: atrioventricular node (node Tahara)
A. Bundle
In muscle fiber connecting directly to the atrium and ventricle, the majority of the accessory pathway is of this type.
Two. Fiber James:
Nodule in the channel between three to contact the sinus node and atrioventricular node (anterior, middle, posterior internodal tracts), the tract between the posterior tubercle is out of the trailing edge of the sinu
s node, atrioventricular node bypass the majority of the often If you have, in conjunction with the normal conduction system in its lower stimulation, which form part of the circular road excitement.
Muscle fibers to ventricular muscle directly linked to the atrioventricular node, bundle of His, from the upper leg.
Extend / shorten the PR interval QRS interval delta wave
Fiber James - + -
Bundle Mahaim + - (or +) +
Nine. Treatment of WPW syndrome
Treatment of WPW syndrome, the treatment (1) of tachycardia attack, divided into two types of radical treatment (2).
Treatment 1) of tachycardia attack
As a treatment during an attack of paroxysmal supraventricular tachycardia has something like the following.
a. Carotid sinus massage: the first is right when, invalid does the left carotid sinus massage.
b. Eyeball pressure: the first is when right, they are deactivated and pressure on the eyeball on the left.
c. You let your breath and close the glottis called Operation: Valsalva.
d. Operation Mueller: to close the glottis, causes sucked the breath.
The fast-acting intravenous drugs such as digitalis Desuranoshido; law pharmacological stimulation of the vagus nerve (2).
The intravenously injected immediately within 3 seconds of 5 ~ 10mg; (10,20,40 mg 2ml); intravenous therapy (3) ATP
Anti-arrhythmic drugs (4)
a. The 5mg intravenously over 5 min once: verapamil (2ml, 5mg Vasolan).
b. Intravenous injection over 3 minutes times 10 ~ 20mg 1: (10,50 mg Herbesser tube 1) diltiazem.
c. By slow intravenous injection at a rate of 50 ~ 100mg / a 500 ~ 1,000 mg: (125,250 mg Amisarin tube 1) procainamide.
d. Intravenous injection over 5 min 1.5 ~ 2mg/kg: disopyramide (5ml, 50mg tube Rythmodan P1).
e. Intravenous injection over 5 min 1.5mg/kg: cibenzoline (5ml, 70mg tube Shibenoru 1).
Perform frequent atrial pacing: atrial pacing (5).
DC shock therapy (6)
Radical treatment of the syndrome 2) WPW
On admission to estimate the position of the accessory pathway by cardiac electrophysiological testing, and energized by high-frequ
ency current ablation using a catheter electrode that site. Equipment recently, the success rate significantly improved by advances in diagnostic techniques, now the standard treatment of WPW syndrome now.
Success rate of ablation accessory conduction pathway, but depends on the site location of the accessory pathway, in the accessory pathway left ventricular free wall was 91% in the conduction pathway 隔副 in 87%, right ventricular free wall and depends on the investigation of the NASPE in the accessory pathway is the success rate of 82% has been reported. Incidence of complications was 2.1%, the mortality rate is 0.2%. Recently, the facility also further improved the success rate, that increase the success rate of 95% or more, serious complication is no longer seen.
Prevention of tachycardia attack by three oral drugs)
In the case of motion and tachycardia
a. Verapamil (40mg tablets Vasolan 1) Date: 120 ~ 240mg /, 3 minutes
b. Flecainide (50,100 mg tablet Tanbokoru 1) Date: 100 ~ 200mg /, 2 minutes
c. Pirushikainido (25,50 mg tablets a San rhythm) Date: 150mg /, 3 minutes
d. Disopyramide (150mg tablets Rythmodan R1): Sun 300mg /, 2 minutes
e. Propafenone (100,150 mg tablet Puronon 1) Date: 300mg /, 3 minutes
f. Cibenzoline (50,100 mg tablet Shibenoru 1) Date: 300 ~ 450mg /, 3 minutes
Treatment during an attack of paroxysmal atrial fibrillation 4)
Antiarrhythmic drug therapy (1)
a. 500 ~ 1,000 mg intravenously at a rate of 50 ~ 100mg /: procainamide
b. Disopyramide: 1.5 ~ 2mg/kg, IV slowly
c. Cibenzoline: 1.5mg/kg, intravenously slowly
Mosquito sinus rhythm by a single dose of anti-arrhythmic drugs (2)
a. Only a single oral 100mg: (25,50 mg per tablet) San rhythm
15 cases of attempt to paroxysmal atrial fibrillation, the success (in the case within 7 days of onset of success to 92%) to over 73% of sinus rhythm.
As a side effect, it has admitted more than four seconds of cardiac arrest in two patients.
b. 200mg (The following persons 60kg weight 150mg) oral only once: (50,100 mg per tablet) Pimenoru. 44% rate of sinus rhythm.
I think a single dose of anti-arrhythmic drugs for these paroxysmal atrial fibrillation, and it is necessary that on top of the hospitalization, carried out by cardiologists under ECG monitor
.
Comments
Post a Comment